Supported By



Leukemia is a cancer of the blood and bone marrow. Bone marrow is the spongy, soft center of bones where stem cells are formed. Some stem cells in the bone marrow mature to form different types of blood cells:
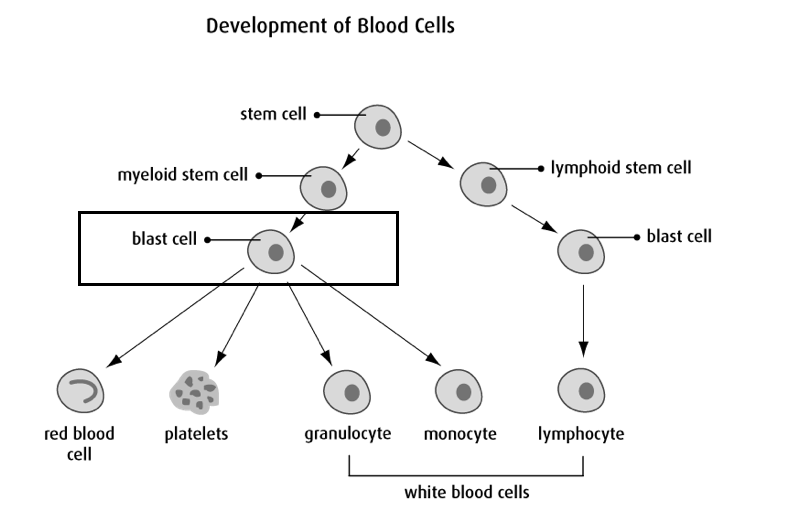
Cancer is the uncontrolled growth of abnormal cells in your body that can cause damage to other organs and tissues. In acute myeloid leukemia (AML), it is the uncontrolled growth of immature, abnormal blood cells sometimes called “blast cells” (see diagram above). It is normal for a small number of blast cells to be present in the bone marrow, but in case of AML a large number of abnormal blasts cells start to overtake the bone marrow.
Patients suspected of having AML require a bone marrow biopsy for confirmation of diagnosis. A bone marrow biopsy is a procedure in which a small sample of bone and bone marrow are collected from your bone. Please see Diagnostic Tests and Procedures for more information.
Note: We are attempting to provide patients with information on the most common treatment utilized; however, it is ultimately up to the Transplant Physician to determine the safest recommended course of action for each individual patient.
Chemotherapy medications are anti-cancer drugs that can be injected into a vein or muscle or taken by mouth, in an attempt to control or kill cancer cells. These drugs enter the bloodstream and spread throughout the body. The chemotherapies that are prescribed have been very carefully planned as part of a protocol just for you. Before your treatment begins, your physician will review the risks and benefits with, then ask you to sign an informed consent.
Chemotherapy is an important part of your treatment and will consist of one or more different types of medications depending on the type of disease you have. The chemotherapy is given on a special schedule that is thought to be best for killing your cancer cells while minimizing the harm your body. Your doctor will discuss with you what days you will receive chemotherapy, the type of chemotherapy and how you should expect to feel.
Younger patients with AML are usually treated with induction chemotherapy, usually requiring 2 types of intravenous (IV) chemotherapy: one given for 3 days and one given for 7 days. You will hear this commonly referred to as “7+3” chemotherapy.
The goal of “induction” chemotherapy is to “induce” a complete remission and another bone marrow biopsy will be done around 4 weeks after starting treatment to determine if the patient is in complete remission. Complete remission is achieved when there is less than 5% blasts in the bone marrow and normal recovery of blood counts. After complete remission is achieved, further chemotherapy treatment, called consolidation chemotherapy, is given to attempt to cure the leukemia. Consolidation chemotherapy is usually given in 2-3 cycles and can be administered in the inpatient or outpatient settings. If a patient does not achieve remission, or the leukemic cells return, more chemotherapy treatment will be required.
If your physician has informed you that you will be receiving 7+3 induction chemotherapy, you can download and reference the module below for more thorough information regarding this chemotherapy treatment.
All-Trans Retinoic Acid (ATRA)
ATRA, a derivative of Vitamin A, is a highly effective treatment for the M3 variant of AML, also known as acute promyelocytic leukemia or APL. ATRA is NOT a useful drug for other forms of AML.
Arsenic Trioxide
Arsenic compounds have shown to be effective in acute promyelocytic leukemia. It is commonly given in combination with ATRA as induction chemotherapy for APL.
In some cases, a stem cell transplant may also be considered after remission to try and cure the leukemia. Generally, stem cell transplant offers a better chance of preventing the leukemia from returning than chemotherapy alone but it is also a more risky treatment that can lead to more complications and side-effects. The decision of whether or not to undergo stem cell transplant can be complicated and AML patients and physicians will discuss the pros and cons of this approach.
Stem cells are “baby cells” that can grow into many different types of cells. They are able to recognize what type of cells require replacement in the body, and will mature into this particular cell. A stem cell transplant may be used for some patients with AML to try to replace the patient’s cancer cells with a donor’s healthy stem cells.
If an individual is a candidate for a transplant, patients with AML receive an allogeneic stem cell transplant. Allogeneic refers to the type of transplant where stem cells are collected from a donor, either a relative or a volunteer donor. The donor stem cells can be collected from the donor’s bone marrow or the blood; however, it is more common practice to collect stem cells from the donor’s blood as it is a less invasive procedure.
The transplant itself is also a non-invasive procedure. The stem cells will be infused into the patient through an IV line that goes into their bloodstream. A nurse will be administering the stem cell transplant and they will remain with the patient the whole time. The infusion of cells generally takes only 30 minutes to 1 hour.
Note: A stem cell transplant may not be an appropriate treatment option for some patients, and therefore not all patients with AML will receive one.
If your Transplant Physician has informed you that you are going to receive a stem cell transplant, you can download and reference the module below to obtain more thorough information regarding the allogeneic transplant process.
Most people find it helpful to have information about side effects so they know what to expect and how to manage them. Although the side effects of treatment can be unpleasant, it is important to know that they are usually temporary. Many of these side effects and complications can be treated with medications and careful monitoring.
Remember that all patients are unique. No two persons will have the same experience with side effects. The degree and intensity of each possible side effect also vary greatly from person to person.
Your BMT healthcare team will work closely with you to minimise any discomfort that you may have as a result of your treatment.
During your therapy, the nurses and doctors will refer to your blood counts. These are the cells in your blood stream that are made by your bone marrow, the factory of all our blood cells. Chemotherapy affects the bone marrow’s ability to make these cells.
The blood counts to which the nurses and doctors will refer are the hemoglobin, platelets, and neutrophils. Let’s discuss each one of them:
1. Hemoglobin:
Anemia is a condition in which you don’t have enough healthy red blood cells to carry adequate oxygen to the body’s tissues. The blood count that measures our anemia is hemoglobin.
Some treatments can reduce your red blood cells and cause anemia. You may feel very tired, weak, dizzy or short of breath. You may notice that your skin, gums, and nails are pale. The symptoms will improve as your body produces more red blood cells. We monitor your hemoglobin to tell us how anemic you are, and to determine if you will need a blood transfusion.
What can help with symptoms of anemia:
2. Platelets:
Platelets are cells that help the blood to clot. Some chemotherapy drugs can cause your bone marrow to make fewer platelets. If you have a very low platelet count, you may get symptoms such as:
You may need a platelet transfusion if your platelet count drops too low, or if you are bleeding from low platelets, or before certain invasive procedures.
What can help when you have low platelets:
Call us immediately if you have any of the following:
3. Neutrophils:
Neutrophils are one of the types of white blood cells. These cells are important in protecting you from infection. Chemotherapy will temporarily affect your bone marrow’s ability to make neutrophils. A fever can be a sign of infection. If you have a fever when your neutrophils are low, we may need to act quickly to give you antibiotics to stop a potential infection from causing serious harm.
What you can do to help when you have low neutrophils:
How and When to Take Your Temperature:
Undergoing cancer treatment can affect every part of your life, including your body, feelings, relationships, self-image and sexuality. Some patients say that the emotional impact of treatment can be harder to manage than the physical changes.
Anxiety is feeling afraid, overwhelmed or very worried. Depression may make you feel hopeless, isolated or fearful. If any of these feelings have overwhelmed you, tell your healthcare team. They can refer you to a support group or psychiatrist, or give you medicine that can help.
Some of your required medications may make anxiety or depression worse. It is important to tell us how you feel so that we may adjust these medications if necessary.
What you can do to help:
While you’re receiving treatment, your body needs more energy than usual. Eating helps you heal. Getting enough calories, proteins, vitamins and minerals will help prevent muscle loss.
You may not feel like eating because of nausea, a sore or dry mouth, fatigue, taste changes, stress, or just low appetite.
What you can do to help:
Constipation means you’re not having bowel movements as often as you used to. Your stool becomes hard and dry, and having a bowel movement can be difficult or painful.
Changes in your normal bowel movements may be caused by drug treatments for cancer or other drugs you’re taking to manage the side effects of therapy. Constipation can also happen because you’ve changed your eating habits, you’re drinking less liquid or you’re less active.
What you can do to help:
Diarrhea means you have soft, loose or watery stools. You may also have cramps and bloating or feel an urgent need to have a bowel movement. It is important to tell your healthcare team if you have diarrhea so we can determine the cause and how we can help you best manage it.
What you can do to help:
Nausea is when you are feeling sick to your stomach and feel like you have to throw up (vomit). Many of our chemotherapy drugs, other medications, and some of the toxicities (like mucositis) from chemotherapy can cause nausea and vomiting.
What you can do to help:
Foods and fluids that may be easier to eat:
Avoid foods that can make nausea worse:
When Should I take “As Needed” Anti-Nausea Medications?
Your doctor will prescribe you anti-nausea medications to take “as needed.” They can be given in pill or capsule form or, while you’re in hospital, intravenously (IV).
Anti-nausea medicines work best when you take them before or as you’re starting to feel sick. They may not work as well if you take them just as you are about to throw up (vomit). If you’re feeling nauseated and one medication doesn’t work after an hour, try a different one. Tell your doctor or nurse if these medications do not relieve nausea and vomiting. They can make suggestions or prescribe other medicines.
If you have nausea and vomiting at certain times of the day, take or ask for your anti-nausea medicine at least 30 minutes before that time. For example, if you often have nausea or v with meals, take an anti-nausea medication at least 30 minutes before your meal. If you vomit within 1 hour of taking your anti-nausea pill, you can take another pill.
Anti-nausea medications can cause side effects, including sleepiness, constipation, or diarrhea. Most people feel that these side effects are worth the benefit of having their nausea relieved.
Fatigue is the most common symptom felt by people with cancer. Many factors, in addition to the underlying cancer itself, can contribute to cancer related fatigue. These include anemia, poor nutrition, depression, medication side effects, poor sleep and being less active.
What you can do to help:
• Light exercise such as walking around the block or unit can boost your energy.
Many of our chemotherapy drugs can cause temporary hair loss by interfering with the normal growth of hair follicles. Hair loss can happen anywhere on your body. It may start with gradual thinning of your hair, or hair may come out in clumps. Hair growth resumes when you are done taking chemotherapy.
What you can do to help:
Chemotherapy and some other drugs can cause memory changes (sometimes called “chemo brain” or “chemo fog”). You may notice you’re forgetting things more often, having trouble focusing, or having trouble doing more than one thing at once (multi-tasking). Your memory and concentration will get better after treatment is over, but you may notice problems for a few months or longer after treatment.
What you can do to help:
It can be common to develop a dry or sore mouth several days after chemotherapy. This is referred to as mucositis (“mew-co-SYE-tiss”). You may notice small canker sores on the inside of your cheeks or lips, under your tongue or on the base of your gums.
What can help:
Some of the chemotherapy drugs can damage the long nerves in our body. Symptoms of can be numbness or a tingling (pins and needles) or a burning feeling in your hands or feet. Other symptoms can include constipation, or weak muscles in the hands and feet. Usually, these side effects are temporary. But for some people, they may last for several months or even be permanent. Let your healthcare team know if you have any symptoms of weak muscles, numbness, tingling, or constipation
What can do to help:
Having pain does not necessarily mean that your cancer is progressing or getting worse. A number of our procedures, and therapies can cause pain as a side effect. There are different types of pain, which can be managed with different types of medicines. Your nurses and doctors can help with pain relief and we even have pain specialists and our palliative care team that can help relieve very severe pain.
What you can do to help:
Side effects of treatment (such as hair loss, hormone changes, fatigue and emotional changes) can affect your sexuality and the way you see yourself. Common sexual changes include body image concerns, low sexual desire, vaginal dryness, difficulties with erections, pain during sexual activity, and relationship changes.
What can do to help:
It is safe to have intercourse once your blood cell counts have recovered. Platelets should be higher than 50 and white blood cells should be 1.0 or higher. It’s important to use some sort of birth control to prevent pregnancy while you are receiving cancer treatment. If a pregnancy happens with an egg or sperm that has been damaged by chemotherapy or radiation, there is an increased risk for birth defects.
Suggestions to make sex more comfortable:
Some chemotherapy drugs and radiation can cause skin rashes, redness or darkened colour, itching, dryness, peeling or acne-like blemishes. These skin conditions usually go away once treatment is over. Your healthcare team can suggest a treatment specific to your symptoms.
What you can do to help:
Having trouble sleeping (insomnia) is a common problem during treatment. You may have insomnia if you are unable to fall asleep, wake up often during the night or wake up very early and can’t go back to sleep.
Pain, anxiety, depression and some medicines can affect your sleep. Insomnia makes it harder to cope with other side effects of treatment. It can affect your mood and energy level, cause fatigue and make it hard to think and concentrate.
What you can do to help:
A stem cell transplant comes with its own risk of complications, including:
What is it? An infection is the invasion of harmful bacteria, viruses, and fungi or parasites in your body. These germs can come from an external source (outside the body) or from germs that you may already be carrying in your body.
How common is it? They are very common and can vary from mild to life0treatening.
What is the timeline? You are at the greatest risk in the first few months after transplant, especially while your white blood cells are low. Infections can also happen in the months and even years it takes for your new immune system to mature.
What causes it? Your immune system is weak in the weeks and months after transplant. It could be compared to the immune system of a newborn baby and needs time (12-18 months) to mature and fully protect your body from invading organisms.
What can I do? Take all your prescribed medications (antibiotics, antivirals, antifungals) as instructed, follow our infection control guidelines and let us know immediately if you have any signs of infection (ie: fever, chills, cough).
What is it? GVHD happens when your new donor cells (the “graft”) attack your body’s cells (the “host”). There are 2 different types of graft versus host disease:
How common is it? GVHD is very common. It can vary from mild to life-threatening. Chronic GVHD can impact your quality of life and increase your risk of infections.
What causes it? GVHD occurs when your new donor cells think your own body’s cells are foreign, or don’t belong, and attack them.
Why is GVHD Helpful? GVHD can be beneficial in mild to moderate cases. This is because of something called the “graft-versus-leukemia” (GVL) or “graft-versus-tumour” affect. GVL occurs when new donor cells attack any remaining diseased or cancerous cells in your body. Although this graft-versus-leukemia effect is a form of GVHD, it is helpful because it lowers the chance for your disease to return or “relapse” after the transplant.
What is the timeline? Acute GVHD usually starts in the first few weeks of transplant once your new cells have engrafted, and last up until day 100. Chronic GVHD is typically GVHD occurring any time after the first 100 days of transplant.
What will my health care team do? We give you “anti-rejection” medications before and after your transplant to prevent GVHD. There are medication options to also treat GVHD if it does occur.
What can you do? Take all your prescribed medications as directed, attend all your follow-up appointments, and let your health care team know of any symptoms you notice after your transplant. Protect your skin from the sun and avoid smoking.
Signs of Acute Graft Versus Host Disease:
Graft failure is a rare but life-threatening complication of transplant. This happens when your new donor stem cells do not successfully grow in your body. This usually happens within the first weeks after transplant but can happen anytime. Your doctor will talk to you about options if this happens. In some cases, there is the possibility of having a second stem cell transplant.
A stem cell transplant affects your whole body and can cause mild to severe damage to your organs. These symptoms can appear in the months and sometimes years after transplant and are caused by the chemotherapy, radiation and other necessary medications you received. Infection can also cause damage to your organs.
Heart: Severe heart problems are rare but mild heart problems can be common (i.e. blood pressure changes). Tell your health care team immediately if you have any heart symptoms (chest pain, fast heartbeat, etc)
Bladder: Mild kidney and bladder problems can be common, severe kidney problems are rare. Continue to drink fluids and stay hydrated after transplant and tell your health care team if you notice pain with urination or blood in your urine.
Lung: Lung complications can be caused by treatment but are usually related to an infection. Mild breathing problems can be common, such as temporarily needing a small amount of extra oxygen. Severe breathing problems are rare, such as needing a machine to breathe for you. Look after your lungs with deep breathing exercises, staying active through treatment and avoiding smoking, dust and mold.
Bones: Bone density loss can be a common complication and increases your chances of eventually developing osteoporosis and/or breaking a bone. There are medications to prevent and treat this but good nutrition, regular weight bearing exercise (walking, jogging) and strength training are things you can do to prevent bone density loss.
Hormones: Reduced hormones levels, including the thyroid, pancreas and sex glands, can be a mild but common complication. You may need to take medications to balance these hormone changes.
The medical term for when your blood cells recover is called ‘engraftment’. Engraftment is when your donor’s stem cells begin to make new blood cells. Engraftment usually starts 10-14 days after your stem cell transplant day but can take longer. As your blood counts recover, you will notice the side effects and symptoms from the chemotherapy (and radiation) improve.
Once you’ve been cleared for discharge from the hospital, you’ll continue to be seen as an outpatient in the Leukemia/BMT Daycare Unit up until “Day 100” (100 days after transplant) or longer. Your appointments will be every 1-3 days at first, then gradually less frequent.
Sometimes it may be necessary for you to be readmitted to hospital after being discharged. This is usually related to complications like GVHD and infection. This can feel like a big setback but don’t feel discouraged, it can be relatively common.
As you approach “Day 100” you will repeat many of the tests you had before your transplant, then meet with your attending physician to discuss the results and plan for the future.
Note: Some patients may need to continue to receive treatment in the Daycare unit beyond Day 100.
After Day 100, you’ll be referred to our Long-Term Follow-Up (LFTU) Program. Through the program you will receive individualized support to address your symptoms and long-term side effects after transplant.
Generally, it can take roughly 12-24 months for you to return to a relatively normal lifestyle after transplant. Adjusting to life after your stem cell transplant can feel like a slow recovery. You will likely still have good days and bad days. It will take time for you to step back into your roles, such as being a parent, spouse, employee and friend again. Be patient with yourself as you adjust and recover.
Stem cell transplantation can have long-lasting or late-onset effects on your body and as such you need to be monitored and examined regularly for signs of complications. The L/BMT Program of BC offers long-term follow up care through our comprehensive program.
The LTFU Program can offer you support, treatment and education post-transplant. The LTFU team consists of a multidisciplinary team of healthcare providers who specialize in oncology care. The clinic focuses on identifying, preventing, and managing any long-term and late effects associated with transplant. Your visits will involve assessment and management of complications or issues you may be experiencing, and development of a plan to support your future health.
If you have any questions that cannot be answered by your personal doctor or if you and your doctor have determined that consultation from the LTFU Program is needed, we are here to help. Patients who have lost contact with the Leukemia/BMT Program of BC after their transplant are also encouraged to get in touch with us. To reach us Monday through Friday during the hours of 0800 until 1600 call (604) 875-4111 ext. 64335 or email LTFU@bccancer.bc.ca. For emergencies, please call 911 or go to your nearest emergency department.